
Ageing of the body predisposes to a high incidence of undernutrition in the elderly person regardless of where he or she is living, but the prevalence of malnutrition is particularly high in hospitalized or institutionalized patients. Numerous conditions in relationship with physiological ageing, comorbidity, polymedication, and the way of life of the individual predispose individuals to undernutrition. 1 Ageing is associated with an increased risk of malnutrition, decreased nutrient intake, unintentional weight loss and sarcopenia, that all lead to frailty, functional disabilities, and increased mortality. 2 Sarcopenia, an aging-induced generalized decrease in muscle mass, strength, and function, is known to affect elderly individuals by decreasing mobile function and increasing frailty and imbalance that lead to falls and fragility fractures. Sarcopenia has been reported to affect more than 40% of elderly individuals older than 70 years of age, approximately 50 million people worldwide. This number is estimated to increase to 500 million people by the year of 2050. 3
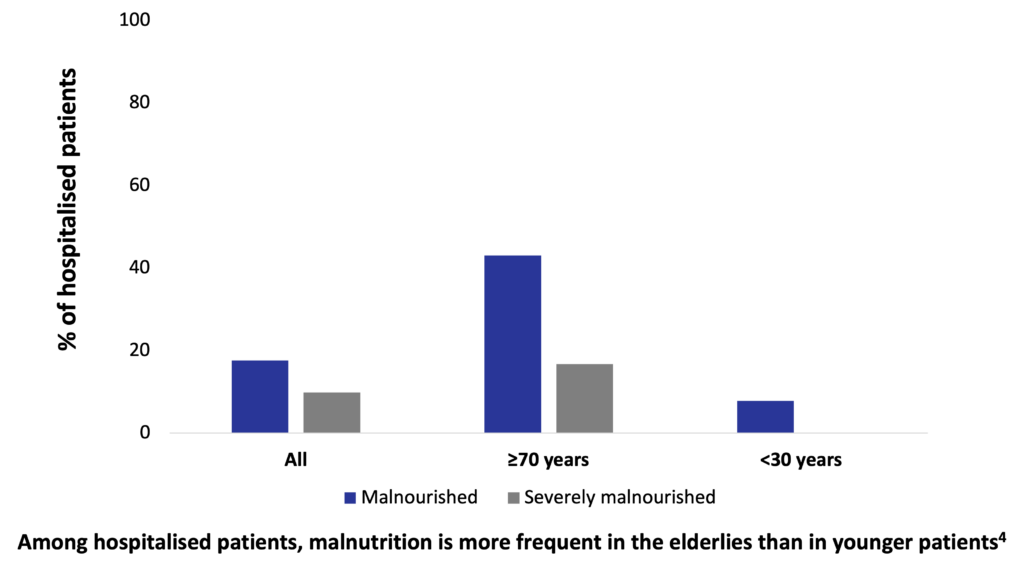
A German hospital malnutrition study conducted in 1,886 consecutively admitted patients in 13 hospitals found that 27.4% of these patients were malnourished, based on subjective global assessment: 17.6% were classified as moderately malnourished, and 9.8% as severely malnourished. Of patients aged ≥70 years, 43% were malnourished, with 16.7% classified as severely malnourished. In comparison, only 7.8% of patients aged <30 years were malnourished, and none were classified as severely malnourished. The highest prevalence of malnutrition was found in geriatric departments, followed by oncology and gastroenterology departments. Malnutrition was associated with a 43% increase of hospital stay. 4
Age-related cognitive decline is a main predictor of disability among elderly people, and with the continued expansion of the aging population and the increase in life expectancy, the prevalence of mild cognitive impairment and dementia have increased. 5 Alzheimer disease or dementia is prevalent in both nursing facilities and in assisted living / residential care communities, where it affects 45% of older adults. 6
Risk factors of protein–energy malnutrition are poor appetite, edentulousness, having no diabetes, hospitalization and poor self-reported health.7 Sarcopenia is believed to be caused by multiple factors such as disuse, malnutrition, age-related cellular changes, apoptosis, and genetic predisposition. The etiology of sarcopenia comprises a wide variety of causes that are involved in a complex manner, including disuse secondary to comorbidities (e.g. malnutrition, vitamin D deficiency, cerebral infarction, heart failure, and osteoarthritis) as well as age–related hormonal changes, denervation, changes in inflammation and immunity, social causes, and mental causes such as decline in cognitive function or decrease in social activity.8
There are a variety of nutritional factors, including nutritional status and dietary patterns, that might be associated with cognitive function, and specific micronutrients and dietary components have been suggested to have an association with cognitive function as well.9 It has been shown that frequency of malnutrition in patients with mild cognitive impairment is significantly higher than in patients with normal cognition, and is not significantly different from that in patients with dementia. 10
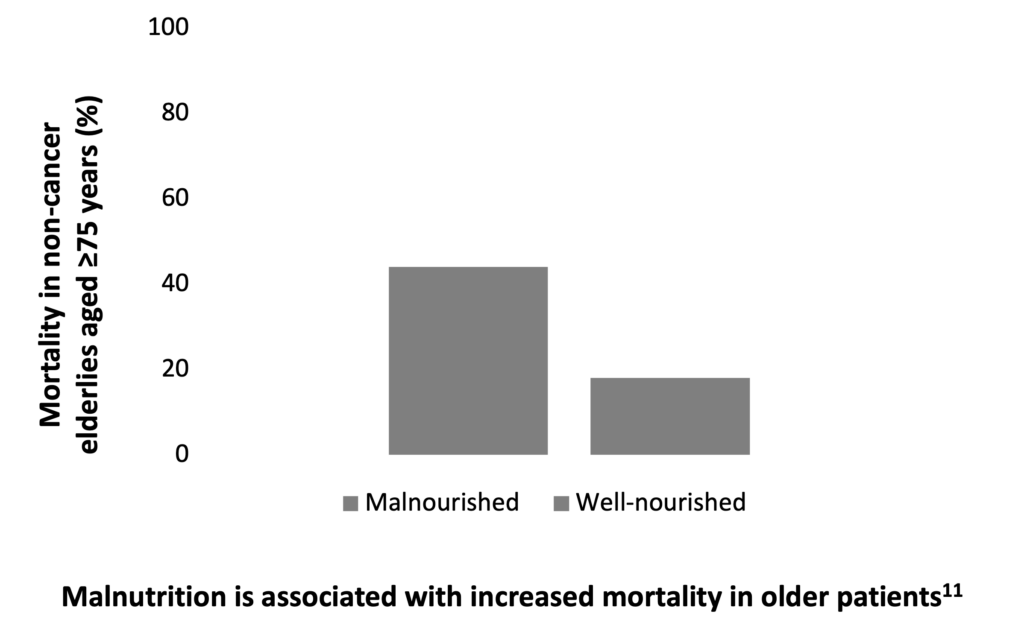
Protein-energy malnutrition is associated with numerous poor health outcomes, including high health care costs, mortality rates and poor physical functioning in older adults.7 A study of 205 non-cancer elderly patients aged 75 years or older showed that protein-energy malnutrition is associated with an increased mortality in this patient population. 11
Getting the right amount of nutrients is crucial for preventing weight loss and muscle wasting to keep up strength, and to overcome weakness caused by the disease-related malnutrition. A high calorie diet has been shown to induce weight gain, increase BMI, and improve clinical outcomes, such as cognitive functions in older patients with dementia. 12
Most elderly subjects have insufficient caloric and protein intake.. Due to the multifactorial etiology of sarcopenia in elderlies, the development of a specific treatment is quite difficult and evidence of effective treatment is limited. One of the therapeutic methods that are currently being attempted is nutritional therapy. Dietary intervention based on nutritional supplement drinks containing proteins, and exercise therapy resulted in improved muscle strength in elderly women.3 Moreover, regular courses of oral supplementation may help maintain the increase in fat-free mass and improve the nutritional status of older patients.13
Although oral nutritional supplements are known to be effective to treat malnutrition in the elderly, a known barrier for oral nutritional supplements use among elderly is the volume that needs to be consumed, resulting in low compliance and thus reduced effectiveness. A randomized controlled intervention trial of elderly nursing home residents with high functional impairment showed that a low-volume, nutrient- and energy-dense oral nutritional supplement was well accepted and resulted in significant improvements of nutritional status and, thus, was effective to support treatment of malnutrition.14
References:
- Allepaerts S. et al. [Nutrition in the elderly]. Rev Med Liege 2014;69:244-50.
- Suominen MH. et al. Nutritional guidelines for older people in Finland. J Nutr Health Aging 2014;18:861-7.
- Hida T. et al. Managing sarcopenia and its related-fractures to improve quality of life in geriatric populations. Aging Dis 2013;5:226-37.
- Pirlich M et al. The German hospital malnutrition study. Clin Nutr 2006;25:563-72.
- Ogawa S. Nutritional management of older adults with cognitive decline and dementia. Geriatr Gerontol Int 2014;Suppl2:17-22.
- Posthauer ME. et al. Enteral Nutrition for Older Adults in Healthcare Communities. Nutr Clin Pract 2014;29:445-8.
- van der Pols-Vijlbrief R. et al. Determinants of protein-energy malnutrition in community-dwelling older adults: A systematic review of observational studies. Ageing Res Rev 2014;18C:112-31.
- Hida T. et al. Managing sarcopenia and its related-fractures to improve quality of life in geriatric populations. Aging Dis 2013;5:226-37.
- Ogawa S. Nutritional management of older adults with cognitive decline and dementia. Geriatr Gerontol Int 2014;Suppl2:17-22.
- Orsitto G. et al. Nutritional status in hospitalized elderly patients with mild cognitive impairment. Clin Nutr 2009;28:100-2.
- Cederholm T. et al. Outcome of protein-energy malnutrition in elderly medical patients. Am J Med 1995;98:67-74.
- Allen V. et al. The influence of nutritional supplement drinks on providing adequate calorie and protein intake in older adults with dementia.
Clin Nutr 2013;17:752-5. - Lauque S. et al. Improvement of weight and fat-free mass with oral nutritional supplementation in patients with Alzheimer’s disease at risk of malnutrition: a prospective randomized study. J Am Geriatr Soc 2004;52:1702-7.
- Stange I. et al. Effects of a low-volume, nutrient- and energy-dense oral nutritional supplement on nutritional and functional status: a randomized, controlled trial in nursing home residents. J Am Med Dir Assoc 2013;14:628.e1-8.